Your cart is currently empty!
Articles/News
MTHFR debunked

This fascinating article explains in detail many of the wrong assumptions of the so-called MTHFR-experts. It shows why some of their assumptions are based on facts almost pulled out of thin air. And it raises the question of how they can be sure about suggesting supplements based on single mutations. We look at the science behind it. One assumption among “MTHFR-experts” is that homozygous mutation in MTHFR C677T results in enzyme activity reduction of 70%. This exact number is far from proven. Besides, the very uncertain underlying scientific findings of activity reduction is even misinterpreted to the claim that 70% less methylfolate is produced! There are more than 100 SNP locations in MTHFR. MTHFR consists of about 600 amino acids and is a relatively large enzyme. 677 and 1298 are just two of these locations (SNPs) that are thought to be more significant than others, but “MTHFR-experts” seem to convince us that these two SNPs in MTHFR are the only ones there are (OK, they are considered the two most important locations, but…). Consider this fact when you look at a “genetic report” showing only locations 677 and 1298. If you have a mutation in one (or both) of these two, you still have around 100 MTHFR locations that might work at 100% efficiency if there are no SNPs in these. Or you might have mutations in many of these locations not showing in the genetic report.
Another assumption from the “experts” is that the same mutation results in folate deficiency, and that is far from the truth in most cases (based on the alternative fact that you produce up to 70% less methylfolate when you have a double C677T mutation). If you read on, you will find the underlying scientific findings the “experts” use does not prove that at all. You should also read our BLOG-post “Methylfolate – the “suicidal” nutrient (don’t believe the hype).” Some even recommend multivitamins, eating folate-rich foods or even take folate supplements, and that could make things even worse. Folate is not better than folic acid, and methylfolate is just slightly better. The assumption that one “cannot” convert folic acid, and only convert naturally occurring folate, is entirely wrong. Too much of any of these (even methylfolate) could be a problem, but not for these reasons. Detoxing also seems to be a focus, but why not address the cause of the problem, which is poor methylation, by taking SAMe and cofactors instead of a bunch of alternative detoxing activities only? Of course, living a healthy lifestyle is also important. Besides, MTHFR does not mean that you are under-methylated (even if most maybe are), you could also be over-methylated (even if that is rarer), and that results in diametrically different symptoms and needs. “MTHFR-experts” might give you the impression that MTHFR mutants are one homogeneous population with the same “disease”, and that taking a genetic test will give you many answers. What they don’t tell you is that it just gives you a lot of questions and confusion. This makes you more susceptible to their simple or complex explanations and recommendations since they are the experts, and if you have that single mutation, everything can be explained.
The exact number of genes in the human genome is not even found yet (estimates at the time being around 20,000), and we all have thousands of mutations (heterozygous or homozygous). One mutation does not at all mean the gene/enzyme is not working at all! The efficiency of the enzyme might be reduced, but maybe not as much as some would like you to think. We are all different, and that is a good thing. Variation is crucial for health and evolution, and most mutations have advantages as well as disadvantages making us all distinct in some way or another. Even identical twins who shared the same DNA at conception will have different genes (mutations) at birth and even develop differences later in life. This is called epigenetic changes (gene expression), and it turns out that methylation plays one of the most important roles in this:
http://www.walshinstitute.org/epigenetics.html
“In general, methylation tends to inhibit or prevent gene expression, and the absence of a methyl mark tends to promote expression. Once established in the womb, the marks are firmly in place and usually persist throughout life. Environmental insults can produce deviant marks in the womb or later in life. Although the technology for reversing deviant bookmarks is still unavailable, effective therapies for the treatment of many epigenetic disorders are known today. For example, many paranoid schizophrenics exhibit excessive dopamine activity that can be normalized by Vitamin B-3 that uncoils DNA to increase gene expression of DAT proteins (comment: this is the case for over-methylation). In another example, methionine and SAMe act as serotonin reuptake inhibitors by compacting chromatin to reduce production of SERT transport proteins. (comment: this is the case for undermethylation)”.Many of the facts on this website https://VITAcure.me are based on the research of the non-profit organization Walsh Research Institute. For more information about the Walsh Approach, we encourage you to read the book “Nutrient Power” by the founder and President of the Walsh Research Institute, William J. Walsh, Ph.D., FACN.
Every “MTHFR-expert”, and also other good neutral sources, claiming that enzyme activity is reduced by up to 70% (only when you are homozygous for MTHFR C677T, and much less when heterozygous) all use as evidence this article from 1994 (or links referring to it):
http://digitalcommons.unl.edu/cgi/viewcontent.cgi?article=1123&context=lawfacpub
The fact is that the level of enzyme activity reduction is not proven with certainty, and could be far from accurate or even very wrong due to some extraordinary conditions during the experiment. Even if it was correct it should not scare you, since you still have many other locations in MTHFR enzyme and other enzymes working at 100%, and supplementing with only methylfolate and too much of it could make things even worse especially if folate level is high. They also mention that in this article from 1994: “Large case-control studies are required to evaluate the frequency of this genetic change… And …Well-defined populations need to be examined, as the limited data set thus far suggests that population-specific allele frequencies may exist” (and while we are waiting for these studies, some still use it as proof).
In this study, there were only five people who were homozygous for MTHFR C677T chosen from another study with vascular diseases, and another seven individuals from another group (total 12 individuals). That is very few! In the “normal” group (no mutation in MTHFR C677T) there were only 19 people, and in the heterozygous group, there were only nine individuals! The low number of people is only one of the factors contributing to the uselessness of this study. At least one should question why the number 70% is used uncritically without mentioning the limitations in this study.You can still make sure the homocysteine level is not very high, but when undermethylated as most MTHFR mutants are, the homocysteine level is usually low (and it is more important, or at least beneficial to use the homocysteine actively in the methylation cycle). Some other studies suggest that homocysteine could be higher with homozygosity for the C677T (MTHFR 677C>T), and not with not heterozygosity. We will get back to these below, and there are sources of error and extraordinary conditions, but anyway, if homocysteine is higher with this mutation only, there are other vitamins that could alter homocysteine levels (like B6, B12, etc.) as found in the VITAcure Methyl Plus supplement.
Some general studies are suggesting an association between the MTHFR polymorphism and elevation of homocysteine, but this seems like only in studies of Indian population and not in western population, so other nutritional/environmental/genetic factors (or statistical errors) might be the cause:
https://www.ncbi.nlm.nih.gov/pubmed/25591425
As this article from American Heart Association suggests:
http://circ.ahajournals.org/content/132/1/e6
“Mild to moderate homocysteine elevations are common; extremely high homocysteine elevations are uncommon”.
“If I Have Elevated Homocysteine, Should I Be Treated?
No. Although taking a daily supplement of folic acid, vitamin B6, or vitamin B12 can effectively lower blood homocysteine levels; such lowering does not lead to a decreased risk of cardiovascular disease, DVT, or PE. Therefore, at present, such supplementation with folic acid, vitamin B6, or vitamin B12 for primary prevention of heart disease is not recommended. Similarly, treating patients with elevated homocysteine and cardiovascular problems or DVT or PE is also not recommended.”
“In the United States, ≈20% to 40% of white and Hispanic individuals are heterozygous for MTHFR C677T… Although having a reduced enzyme function of MTHFR can lead to elevated homocysteine levels, it does not necessarily do so; many people have normal homocysteine levels” (comment: for this group there is no scientific proof indicating elevated homocysteine, quite the contrary according to sources above, and even if it was the case, the elevation is nothing to worry about).
“The presence of MTHFR mutations does not require any special treatment, such as supplementation with folic acid, vitamin B6, or vitamin B12, and no additional concerns arise.” (Comment: looking at the two MTHFR mutations 677&1298 only has no meaning. You should look at your total symptoms, etc., and perhaps you have a methylation imbalance (more likely), and because of that you are low in certain nutrients, then you should supplement with helpful nutrients to correct this imbalance). The imbalance could be due to many factors, genetics being one, and many genes are playing a role in this (MTHFR genes are only part of the explanation). Nutritional and environmental factors could also explain imbalances (diet, stress, etc.).
We mentioned some studies of homozygous MTHFR C677T. “MTHFR 677C>T polymorphism is the one most extensively investigated. However, the lack of homogeneity in the data and the high number of factors influencing plasma homocysteine concentrations remain conflicting. Moreover, studies on the evaluation of therapeutic interventions in improving the atherogenic profile, lowering plasma homocysteine levels, and preventing vascular events, have shown inconsistent results”.
https://www.ncbi.nlm.nih.gov/pubmed/18670064
“Hyperhomocysteinaemia is a multifactorial disease; smoking, coffee consumption, and lack of exercise can raise tHcy (Refsum et al. 1998; Nygard et al. 1997a; Nygard et al. 1998).”
Here is one Norwegian study it is often referred to (The Hordaland Homocysteine Study). It is an interesting study, but it does not prove that homozygous C677T results in elevated homocysteine (and that is not what they claim in this study either):
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC507663/
“From 1992-93, we screened 18,043 subjects, aged 40-67 yr, and found 67 cases (0.4%) with total plasma homocysteine (tHcy) > or = 40 micromol/liter. Compared to 329 controls, the cases had lower plasma folate and cobalamin levels, lower intake of vitamin supplements, consumed more coffee and were more frequently smokers. Homozygosity for the C677T mutation in the methylenetetrahydrofolate reductase gene was observed in 73.1% of the cases and 10.2% of the controls.”…
“We conclude that most subjects with hyperhomocysteinemia > or = 40 micromol/liter in the general population have the C677T mutation combined with low folate status. A daily supplement of low dose folic acid will reduce and often normalize their tHcy level.”
“Likewise, Jacques et al. (29) demonstrated that individuals who are homozygous for the C677T mutation have elevated tHcy only when the plasma folate is in the lower normal range” (comment: that is usually more often the case with over-methylators as data from Walsh Research Institute shows).
Besides, why would people with homozygous MTHFR C677T have a lower intake of vitamins, consume more coffee and more important: be more frequently smokers? And just THAT could be the whole reason for their vascular problems (first of all the smoking of course, and lack of exercise – coffee drinking is no longer a significant risk factor as regarded in the 90s).There are also other critical sources of errors:
1. The conditions: they did not measure MTHFR activity inside the human body. The DNAs were expressed in E. coli (bacteria) to yield protein, and in addition to that, the extracts were heated to 46 degrees Celcius for five minutes. As they say: “the expression experiments were not designed to measure differences in specific activity before heating since variation in efficiencies of expression could contribute to difficulties in interpretation”. And “It is possible that the mutant protein has increased stability in E. coli (comment: or perhaps the other way round), or that “inclusion bodies” in our extracts contributed to differences in recovery of properly-assembled enzyme.”
2. The selection. For instance, it is not sure at all that a homozygous mutation (in it self) increases the risk for elevated homocysteine levels which again increases the risk for vascular diseases – we will get back to that. Other scientific data from Walsh Research Institute – using a much larger database of more than 30,000 individuals (might be much higher now), shows that elevated homocysteine is more common with over-methylation and that homocysteine usually is low with undermethylation regardless of individual mutations. This could mean that most persons in this study were over-methylated, and therefore also depressed in folates (as confirmed by the study itself):
http://www.walshinstitute.org/biochemical-individuality–nutrition.html
This makes the selection very unusual since MTHFR mutation tends to slow down the methylation cycle. Besides, there are three times as many under-methylated people than over-methylated ones in the total population. Therefore the selection might be unusual in that regard also.
The headline for the article is “Mutation in MTHFR as candidate genetic risk factor for vascular disease.” However, they say “…our experiments do not directly address the relationship between this change and vascular disease. Nonetheless, this mutation represents a diagnostic test for evaluation of MTHFR thermolability in hyperhomocysteinemia”.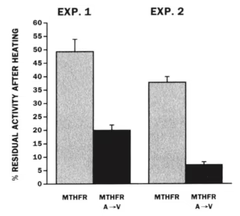
Even if MTHFR activity is lower (although not as much as 70%), that does not at all mean that the enzyme is not working at all, and one is not able to convert folate (as some misinformation out there from “MTHFR-experts” claims). One would simply not be alive if it did not work, and it happens more than a billion times per second for everyone regardless of MTHFR (the process is only a bit slower with some, and a bit faster with others depending on ALL genes active in methylation and also other nutritional and environmental factors).
Severe MTHFR deficiency, however, is extremely rare (only about 50 cases worldwide). It is much more likely that you win first prize in the lottery, and you would also have serious problems that would be discovered without a general screening of MTHFR) and caused by mutations resulting in (perhaps) 0–20% residual enzyme activity:
https://www.ncbi.nlm.nih.gov/pubmed/20356773
If you are homozygous for only one of the two MTHFR genes, you do not need to worry about that in it self, but you should look at the methylation cycle as a whole (if it is slow, fast or normal). Several mutated genes slow down the cycle, for instance: MTHFR, SAHH, BHMT, MS, MAT, etc., and there are mutations in other genes that speed up the cycle: AGAT, GAMT, CBS, MT, etc. It is still too early just by looking at the combinations of these and other genes to find out if you should supplement or not. It is better to look at symptoms or take a blood test measuring SAM/SAH.
Human Study Confirms Potent Antidepressant Effects of SAM-e
Read this interesting study on how SAMe has improved the lives of those showing resistance to antidepressants (From LifeExtension®*):
Human Study Confirms Potent Antidepressant Effects of SAM-e
Life Extension® introduced SAMe (S-Adenosyl-Methionine) in 1997. Back then it was enormously popular in Europe, but unknown in the United States. The National Institute of Mental Health decided to fund a double-blind, placebo-controlled trial that would evaluate SAMe as an additive therapy in those suffering major depression who were resistant to FDA-approved drugs. Researchers at Harvard Medical School and Massachusetts General Hospital gave patients 800mg of SAMe twice daily along with a selective serotonin reuptake inhibiting drug (SSRI).
Relative to placebo, patients who received the SAMe showed a 105% higher response rate and a 121% higher remission rate.(1) Said differently, add-on therapy with SAMe in patients with drug-resistant depression produced double the response rate AND remission rate compared with placebo within a 6-week period.
This study was published in the August 2010 issue of the American Journal of Psychiatry.(1) It was a follow-up to a 2004 pilot study that showed greater benefits when antidepressant drugs were combined with SAMe than when the same drugs were taken alone.(2)
 For the past 13 years, SAMe has been on Life Extension’s TOP TEN list of the most important steps to take to ensure optimal longevity. SAMe has been recommended to aging individuals not to just feel better, but also to protect the brain, liver, joints, and other tissues of the body like no other substance. This article reviews and updates the many studies documenting the anti-aging properties of SAMe.
For the past 13 years, SAMe has been on Life Extension’s TOP TEN list of the most important steps to take to ensure optimal longevity. SAMe has been recommended to aging individuals not to just feel better, but also to protect the brain, liver, joints, and other tissues of the body like no other substance. This article reviews and updates the many studies documenting the anti-aging properties of SAMe.A listing of all the drugs the FDA has approved to treat depression would fill several pages of this magazine. A major problem with these antidepressant drugs is that they fail a significant number of patients—up to 30%, by some accounts.3 In many cases, the drugs make depressed individuals feel worse, and FDA-mandated labeling now requires a warning that use of some antidepressants increases suicide risk—which is an incredible contradiction considering that suicide is a leading cause of death amongst depressives.
An equally disconcerting issue is the many side effects associated with antidepressant medications such as weight gain, constipation, dry mouth, and other symptoms that cause many depressives to stop using them.
There is thus an urgent need for a new approach to treating those who fail to respond to currently available antidepressant medications. Encouraging news from a recent study shows that the addition of S-Adenosyl-L-Methionine (SAMe) to a serotonin reuptake inhibitor drug markedly improves the percentage of severe depressives who are relieved of their disorder.
Unlike synthetic prescription drugs that induce unintended side effects, SAMe is a naturally-occurring agent in the body that performs a multitude of beneficial functions, such as boosting glutathione levels in the brain and liver. The anti-aging properties of SAMe are so profound that non-depressives take it each day (in lower doses) just like they do their other dietary supplements.4,5
Antidepressants Don’t Work
 As a team of Harvard researchers noted in a remarkable 2010 study published in the Journal of Clinical Psychiatry,(6) “The majority of depressed patients will not experience remission when treated with a first-line antidepressant.” In other words, antidepressants don’t really work for most patients. More is needed to help depression’s victims.
As a team of Harvard researchers noted in a remarkable 2010 study published in the Journal of Clinical Psychiatry,(6) “The majority of depressed patients will not experience remission when treated with a first-line antidepressant.” In other words, antidepressants don’t really work for most patients. More is needed to help depression’s victims.This is where SAMe comes in.
In modern high-tech imaging studies of healthy human brains, SAMe produces effects typical of several classes of antidepressant drugs(7)—but unlike those drugs, SAMe has remarkably few side effects and is well-tolerated even in elderly subjects.(8)
People with depression may exhibit a variety of biochemical imbalances, but the most common and best-known has to do with neurotransmitters like serotonin (involved in mood, sleep, appetite, and learning) and norepinephrine (involved in heart rate, blood pressure, and the fight-or-flight response). These chemical messengers belong to a class of molecules known as monoamines, and their synthesis in brain cells is largely controlled by the presence of folic acid, vitamin B12—and SAMe.(9-12) When released into the space between brain cells (the synapse), monoamines exert stimulating or inhibiting effects on postsynaptic neurons.
With too little serotonin or norepinephrine available, the brain cannot sustain a positive mood—and depression results. Virtually all antidepressant drugs work to boost levels of these neurotransmitters within the synapse. And therein lie many of their limitations—and the causes of many of their side effects.(13)
SAMe operates through a completely different mechanism than these drugs. A molecule derived from the sulfur-containing amino acid methionine, SAMe is found in every living cell and plays a central role in cellular function.(14,15) In addition to being required for monoamine synthesis, it also affects cell membrane fluidity, which may in turn influence how well a neuron transmits an electrical signal.(16) Recent studies have shown that SAMe is also involved in the so-called “epigenetic” control of cellular function—the ability of cells to activate or suppress specific genes based on environmental influences—by its effects on proteins associated with chromosomes.(17)
These multi-targeted effects, coupled with an extraordinary safety profile, make SAMe a compelling treatment for a wide variety of brain disorders, from depression and cognitive decline to congenital metabolic dysfunction.(18,19) SAMe crosses the blood-brain barrier, making it readily available to the brain and nervous system.(10) This is vital: SAMe levels in the spinal fluid of depressed individuals have been shown to be significantly lower than those of healthy people.(11)
Animal models of depression shed additional light on how SAMe works in the brain. More than two decades ago Japanese scientists demonstrated a reduction in aggression in rats treated with SAMe as a result of its action in the central nervous system.(20) By the turn of this century, researchers in Italy and Spain showed that SAMe reverses experimentally-induced depression in rats, at a rate faster than that of the prescription antidepressant imipramine, the first tricyclic antidepressant developed and without apparent side effects.(21,22) And in a remarkably detailed study, the Italian group showed that SAMe restored diminished brain levels of “polyamines,” essential brain molecules that are reduced in depressed patients.(23)
In 2007 a team of scientists at the University of Massachusetts launched a study using a combination of SAMe with N-acetyl cysteine (NAC) and acetyl-L-carnitine.(24) Their subjects were aging mice with neurodegeneration similar to Alzheimer’s disease, in which depression is often a major manifestation. The combination rapidly enhanced cognitive function and prevented or reduced aggression in the animals, an effect that was rapidly reversed when the combination was withdrawn. The combination also prevented a decline in levels of the neurotransmitter acetylcholine, while contributing important antioxidant effects as well.
WHAT YOU NEED TO KNOW: SAM-e A landmark study funded by the National Institute of Mental Health revealed that the addition of S-Adenosyl-L-Methionine or SAMe produces compelling results in people taking SSRIs, the majority of whom do not experience relief when taking the drug alone. SAMe is a naturally occurring molecule found in all living cells; it supports a host of chemical functions necessary for normal brain activity. SAMe acts by several distinct and independent mechanisms to target multiple sites of action in brain cells that are involved in producing depression. In clinical trials, SAMe has been shown to be at least as effective as prescription antidepressants, but with far fewer side effects. Because of its strong safety record, SAMe should be part of any regimen for brain health, particularly when depressive symptoms are present—and when prescription drugs alone don’t work. SAMe has also been shown to confer enormous benefits to the brain, liver, and joints, halting and even reversing various degenerative conditions, from osteoarthritis and neurodegeneration to nonalcoholic fatty liver disease. Let’s turn now to the clinical realm and examine how well SAMe actually functions in humans suffering from depression.
SAMe Dramatically Improves Therapeutic Outcomes
Clinical trials have repeatedly demonstrated the benefits of SAMe in patients with major depression in a variety of populations: doses of 400-1,600 mg daily consistently resulted in rapid improvement in depressive symptoms and side effects that were mild and transient.(25-27)
SAMe is even effective in patients previously labeled “nonresponders” to conventional drug treatment.(25) This led first to additional studies of SAMe compared with standard drugs rather than placebos, and later to studies in which SAMe was used in addition to such drugs.
SAMe consistently performs as well as or better than older-generation antidepressants such as imipramine and desipramine, drugs which are highly effective but have an unfavorable safety profile.(28-30) In every case, the side effects of SAMe were trivial or mild. Interestingly, one such study found that regardless of whether patients received SAMe or the drug, their levels of SAMe in blood rose significantly as their depressive symptoms improved.(28)
SUPPORT FOR THE AGING BRAIN
Experts have known for more than a decade that severely reduced brain levels of SAMe are directly linked to Alzheimer’s disease.(1) More recent research reveals a direct correlation between levels of SAMe in the brain and Parkinson’s disease. In aging individuals stricken with Parkinson’s disease, parkinsonian symptoms (including increased levels of neurodegeneration) have been shown to be worse when SAMe levels are low, while the cognitive function is markedly better when levels of SAMe are higher.(2) At the core of SAMe’s ability to support brain function and neuronal health is its role in boosting levels of glutathione (GSH) and enhancing the antioxidant power of superoxide dismutase (SOD).(3) Scientists have noted that these twin capabilities underscore SAMe’s importance as a neuroprotective compound, given the extraordinarily high metabolic activity and energy-intensive demands of both brain cells and neurons.(3) References Morrison LD, Smith DD, Kish SJ. Brain S-adenosylmethionine levels are severely decreased in Alzheimer’s disease. J Neurochem. 1996 Sep;67(3):1328-31. Obeid R, Schadt A, Dillmann U, Kostopoulos P, Fassbender K, Herrmann W. Methylation status and neurodegenerative markers in Parkinson disease. Clin Chem. 2009 Oct;55(10):1852-60. Cavallaro RA, Fuso A, Nicolia V, Scarpa S. S-adenosylmethionine prevents oxidative stress and modulates glutathione metabolism in TgCRND8 mice fed a B-vitamin deficient diet. J Alzheimers Dis. 2010;20(4):997-1002.
correlation between levels of SAMe in the brain and Parkinson’s disease. In aging individuals stricken with Parkinson’s disease, parkinsonian symptoms (including increased levels of neurodegeneration) have been shown to be worse when SAMe levels are low, while the cognitive function is markedly better when levels of SAMe are higher.(2) At the core of SAMe’s ability to support brain function and neuronal health is its role in boosting levels of glutathione (GSH) and enhancing the antioxidant power of superoxide dismutase (SOD).(3) Scientists have noted that these twin capabilities underscore SAMe’s importance as a neuroprotective compound, given the extraordinarily high metabolic activity and energy-intensive demands of both brain cells and neurons.(3) References Morrison LD, Smith DD, Kish SJ. Brain S-adenosylmethionine levels are severely decreased in Alzheimer’s disease. J Neurochem. 1996 Sep;67(3):1328-31. Obeid R, Schadt A, Dillmann U, Kostopoulos P, Fassbender K, Herrmann W. Methylation status and neurodegenerative markers in Parkinson disease. Clin Chem. 2009 Oct;55(10):1852-60. Cavallaro RA, Fuso A, Nicolia V, Scarpa S. S-adenosylmethionine prevents oxidative stress and modulates glutathione metabolism in TgCRND8 mice fed a B-vitamin deficient diet. J Alzheimers Dis. 2010;20(4):997-1002.A study conducted in 1992 demonstrated the benefits of combining SAMe and imipramine for speeding the onset of the drug(31)—a critical benefit since almost all antidepressants take three or more weeks to manifest their effects, during which time patients often become discouraged and may discontinue treatment.
In 2004, a Harvard team of psychiatrists used SAMe in patients who were resistant to treatment with more modern drugs.(2) In this open study design, the Harvard group provided 800-1,600 mg per day of SAMe orally to 30 patients who remained depressed despite adequate doses of their medications. Using even a highly conservative statistical analysis, they found that 50% of these previously resistant patients responded to treatment, with an impressive 43% experiencing complete remission of symptoms.(2) These compelling results prompted the same Harvard group to design a larger study to more rigorously examine SAMe’s benefits in augmenting existing drug treatments.(1,32)
The outcome of this study was revelatory, creating a sensation within the scientific community. The group studied 73 patients who were “non-responders” to standard treatment with selective serotonin reuptake inhibitor (SSRI) antidepressants. Subjects stayed on their SSRI for the entire 6-week study period, and took 800 mg of SAMe, or a placebo, twice daily. Their depressive symptoms were monitored using the standard Hamilton Depression Rating Scale. Thirty-six percent of the supplemented patients responded to treatment, and 26% experienced complete remission of their depression—patients who had not felt any difference with standard medications. The placebo recipients had a much worse response rate; just 18% felt a difference and a dismal 12% experienced complete remission.(1)
ARTHRITIS DEFENSE 
A comprehensive 2002 SAMe study conducted by the US Department of Health and Human Services confirmed SAMe’s power not only to sustain the mood but also to optimize joint function.(1) Clinical trials have shown reduced pain and stiffness in aging individuals stricken with osteoarthritis, while in vitro and animal studies have shown SAMe can stimulate the production of cartilage—a crucial factor in halting and reversing arthritis’s progression.(2) Scientists have even found SAMe to be as effective as ibuprofen at reducing morning stiffness, pain at rest, pain during motion, swelling, “cracking” or “popping” sounds, and limited range of motion in arthritic joints.(3) References Available at: http://www.ncbi.nlm.nih.gov/bookshelf/br.fcgi?book=erta64. Accessed September 22, 2010. Hosea Blewett HJ. Exploring the mechanisms behind S-adenosylmethionine (SAMe) in the treatment of osteoarthritis. Crit Rev Food Sci Nutr. 2008 May;48(5):458-63. Muller-Fassbender H. Double-blind clinical trial of S-adenosylmethionine versus ibuprofen in the treatment of osteoarthritis. Am J Med. 1987 Nov 20;83(5A):81-3.The lead author of the Harvard study, Dr. George Papakostas, noted: “SAMe can be an effective, well-tolerated, and safe adjunctive treatment strategy for serotonin reuptake inhibitor nonresponders with major depressive disorder.”(1)
Summary
A landmark study funded by the National Institute of Mental Health revealed that the addition of S-adenosyl-L-methionine or SAMe produces compelling results in major depression sufferers taking SSRIs, the majority of whom do not experience relief with prescription drugs alone. SAMe is a naturally occurring molecule found in all living cells, where it supports a host of chemical functions necessary for normal brain activity. It has been found to be safe at very high doses. Despite a wealth of data from the early 1990s, SAMe hadn’t found clinical acceptance until very recently, when new, rigorously controlled trials demonstrated its effectiveness in instances where drugs don’t work. Given SAMe’s impressive safety record, virtually anyone suffering from depressive symptoms should consider it, whether currently taking medication or not.
If you have any questions on the scientific content of this article, please call a Life Extension® Wellness Specialist at 1-866-864-3027.
OPTIMAL LIVER PROTECTION SAMe’s extraordinary capacity to protect and enhance liver function has been well-  documented in a wealth of studies. To take one dramatic example, blood alcohol levels among binge drinkers who ingest SAMe at the point of consumption have been shown to be significantly lower than controls.1 In 2010, researchers were able to determine why: SAMe boosts the liver’s alcohol elimination rate by increasing expression of genes within liver cells that are specifically involved in alcohol metabolism.(1) Insufficient levels of SAMe have also been linked to a variety of liver diseases, including nonalcoholic fatty liver disease and nonalcoholic steatohepatitis, both increasingly common disorders characterized by fat deposits in liver tissue that may progress to cirrhosis and full-blown liver failure.(2,3) Scientists believe SAMe supplementation can prevent the onset and progression of these potentially fatal conditions. References Bardag-Gorce F, Oliva J, Wong W, et al. S-adenosyl-L-methionine decreases the peak blood alcohol levels 3h after an acute bolus of ethanol by inducing alcohol metabolizing enzymes in the liver. Exp Mol Pathol. 2010 Sep 7. Wortham M, He L, Gyamfi M, Copple BL, Wan YJ. The transition from fatty liver to NASH associates with SAMe depletion in db/db mice fed a methionine choline-deficient diet. Dig Dis Sci. 2008 Oct;53(10):2761-74. Caballero F, Fernandez A, Matias N, et al. Specific contribution of methionine and choline in nutritional nonalcoholic steatohepatitis: impact on mitochondrial S-adenosyl-L-methionine and glutathione. J Biol Chem. 2010 Jun 11;285(24):18528-36.
documented in a wealth of studies. To take one dramatic example, blood alcohol levels among binge drinkers who ingest SAMe at the point of consumption have been shown to be significantly lower than controls.1 In 2010, researchers were able to determine why: SAMe boosts the liver’s alcohol elimination rate by increasing expression of genes within liver cells that are specifically involved in alcohol metabolism.(1) Insufficient levels of SAMe have also been linked to a variety of liver diseases, including nonalcoholic fatty liver disease and nonalcoholic steatohepatitis, both increasingly common disorders characterized by fat deposits in liver tissue that may progress to cirrhosis and full-blown liver failure.(2,3) Scientists believe SAMe supplementation can prevent the onset and progression of these potentially fatal conditions. References Bardag-Gorce F, Oliva J, Wong W, et al. S-adenosyl-L-methionine decreases the peak blood alcohol levels 3h after an acute bolus of ethanol by inducing alcohol metabolizing enzymes in the liver. Exp Mol Pathol. 2010 Sep 7. Wortham M, He L, Gyamfi M, Copple BL, Wan YJ. The transition from fatty liver to NASH associates with SAMe depletion in db/db mice fed a methionine choline-deficient diet. Dig Dis Sci. 2008 Oct;53(10):2761-74. Caballero F, Fernandez A, Matias N, et al. Specific contribution of methionine and choline in nutritional nonalcoholic steatohepatitis: impact on mitochondrial S-adenosyl-L-methionine and glutathione. J Biol Chem. 2010 Jun 11;285(24):18528-36.HARVARD CLINICAL TRIALS OF SAM-e In a recent study published in the American Journal of Psychiatry, the results of a clinical trial conducted at Harvard Medical School and Massachusetts General Hospital were  announced. The researchers found a significant benefit in male and female patients taking S-adenosyl-L-methionine (SAMe) as an additive therapy to treat major depressive disorders.(1)
announced. The researchers found a significant benefit in male and female patients taking S-adenosyl-L-methionine (SAMe) as an additive therapy to treat major depressive disorders.(1)
What made the findings of this study so remarkable is that this favorable response was observed in those who had already failed to respond to standard antidepressant drugs.(1) This double-blind, randomized controlled trial to evaluate SAMe as an additive therapy against major depression in this drug-resistant population was funded by The National Institute of Mental Health.(1) The trial is a follow-up to a smaller study in 2004 that found a greater benefit when antidepressant drugs were combined with SAMe than when these drugs were used alone.(2) In the current investigation, Harvard Medical School researchers assigned adult depressives taking serotonin reuptake inhibitor drugs (like Prozac®, Effexor®, Celexa®, Zoloft®, Paxil®, and Cymbalta®) to receive 800 mg SAMe or a placebo twice per day for six weeks. Those who received SAMe experienced a 36.1% response rate and a 25.8% remission rate, compared to a 17.6% and a 11.7% response and remission rate in the placebo group.1 This translates into a beneficial response and remission rate that was double for those receiving SAMe compared with placebo. An accompanying editorial written by University of California-San Francisco professor of psychiatry J. Craig Nelson, MD stated that the Harvard findings are “persuasive” and that “SAMe offers a novel mechanism of treatment action and opens up a new area for future exploration.” (3) References Papakostas GI, Mischoulon D, Shyu I, Alpert JE, Fava M. S-adenosyl-L- methionine (SAMe) augmentation of serotonin reuptake inhibitors for antidepressant nonresponders with major depressive disorder: a double-blind, randomized clinical trial. Am J Psychiatry. 2010 Aug;167(8):942-8. Alpert JE, Papakostas G, Mischoulon D, et al. S-adenosyl-L-methionine (SAMe) as an adjunct for resistant major depressive disorder: an open trial following partial or nonresponse to selective serotonin reuptake inhibitors or venlafaxine. J Clin Psychopharmacol. 2004 Dec;24(6):661-4. Nelson JC. S-adenosyl-L-methionine (SAMe) augmentation in major depressive disorder. Am J Psychiatry. 2010 Aug;167(8):889-91.References
- Papakostas GI, Mischoulon D, Shyu I, Alpert JE, Fava M. S-adenosyl-L- methionine (SAMe) augmentation of serotonin reuptake inhibitors for antidepressant nonresponders with major depressive disorder: a double-blind, randomized clinical trial. Am J Psychiatry. 2010 Aug;167(8):942-8.
- Alpert JE, Papakostas G, Mischoulon D, et al. S-adenosyl-L-methionine (SAMe) as an adjunct for resistant major depressive disorder: an open trial following partial or nonresponse to selective serotonin reuptake inhibitors or venlafaxine. J Clin Psychopharmacol. 2004 Dec;24(6):661-4.
- Perovic B, Jovanovic M, Miljkovic B, Vezmar S. Getting the balance right: Established and emerging therapies for major depressive disorders. Neuropsychiatr Dis Treat. 2010 Sep 7;6:343-64.
- Panza F, Frisardi V, Capurso C, et al. Polyunsaturated fatty acid and S-adenosylmethionine supplementation in predementia syndromes and Alzheimer’s disease: a review. ScientificWorldJournal. 2009 May 22;9:373-89.
- Gregory PJ, Sperry M, Wilson AF. Dietary supplements for osteoarthritis. Am Fam Physician. 2008 Jan 15;77(2):177-84.
- Fava M. Switching treatments for complicated depression. J Clin Psychiatry. 2010 Feb;71(2):e04.
- Saletu B, Anderer P, Di Padova C, Assandri A, Saletu-Zyhlarz GM. Electrophysiological neuroimaging of the central effects of S-adenosyl-L-methionine by mapping of electroencephalograms and event-related potentials and low-resolution brain electromagnetic tomography. Am J Clin Nutr. 2002 Nov;76(5):1162S-71S.
- Saletu B, Anderer P, Linzmayer L, et al. Pharmacodynamic studies on the central mode of action of S-adenosyl-L-methionine (SAMe) infusions in elderly subjects, utilizing EEG mapping and psychometry. J Neural Transm. 2002 Dec;109(12):1505-26.
- Miller AL. The methylation, neurotransmitter, and antioxidant connections between folate and depression. Altern Med Rev. 2008 Sep;13(3):216-26.
- Carney MW, Toone BK, Reynolds EH. S-adenosyl-L-methionine and affective disorder. Am J Med. 1987 Nov 20;83(5A):104-6.
- Bottiglieri T, Laundy M, Crellin R, Toone BK, Carney MW, Reynolds EH. Homocysteine, folate, methylation, and monoamine metabolism in depression. J Neurol Neurosurg Psychiatry. 2000 Aug;69(2):228-32.
- Herrmann W, Obeid R. Biomarkers of folate and vitamin B(12) status in cerebrospinal fluid. Clin Chem Lab Med. 2007;45(12):1614-20.
- Racagni G, Popoli M. The pharmacological properties of antidepressants. Int Clin Psychopharmacol. 2010 May;25(3):117-31.
- Bottiglieri T. S-Adenosyl-L-methionine (SAMe): from the bench to the bedside–molecular basis of a pleiotrophic molecule. Am J Clin Nutr. 2002 Nov;76(5):1151S-7S.
- Scott JM, Molloy AM, Kennedy DG, Kennedy S, Weir DG. Effects of the disruption of transmethylation in the central nervous system: an animal model. Acta Neurol Scand Suppl. 1994;154:27-31.
- Baldessarini RJ. Neuropharmacology of S-adenosyl-L-methionine. Am J Med. 1987 Nov 20;83(5A):95-103.
- McGowan PO, Kato T. Epigenetics in mood disorders. Environ Health Prev Med. 2008 Jan;13(1):16-24.
- Bottiglieri T, Hyland K, Reynolds EH. The clinical potential of ademetionine (S-adenosyl-L-methionine) in neurological disorders. Drugs. 1994 Aug;48(2):137-52.
- Paul RT, McDonnell AP, Kelly CB. Folic acid: neurochemistry, metabolism and relationship to depression. Hum Psychopharmacol. 2004 Oct;19(7):477-88.
- Yamamoto T, Yatsugi S, Ohno M, Ueki S. Inhibition of mouse-killing behavior by S-adenosyl-L-methionine in midbrain raphe-lesioned and olfactory-bulbectomized rats. Pharmacol Biochem Behav. 1989 Oct;34(2):395-8.
- Benelli A, Filaferro M, Bertolini A, Genedani S. Influence of S-adenosyl-L-methionine on chronic mild stress-induced anhedonia in castrated rats. Br J Pharmacol. 1999 Jun;127(3):645-54.
- Bellido I, Gomez-Luque A, Plaza A, Rius F, Ortiz P, Sanchez de la Cuesta F. S-adenosyl-L-methionine prevents 5-HT(1A) receptors up-regulation induced by acute imipramine in the frontal cortex of the rat. Neurosci Lett. 2002 Mar 15;321(1-2):110-4.
- Genedani S, Saltini S, Benelli A, Filaferro M, Bertolini A. Influence of SAMe on the modifications of brain polyamine levels in an animal model of depression. Neuroreport. 2001 Dec 21;12(18):3939-42.
- Chan A, Shea TB. Effects of dietary supplementation with N-acetyl cysteine, acetyl-L-carnitine and S-adenosyl-L-methionine on cognitive performance and aggression in normal mice and mice expressing human ApoE4. Neuromolecular Med. 2007;9(3):264-9.
- Rosenbaum JF, Fava M, Falk WE, et al. The antidepressant potential of oral S-adenosyl-l-methionine. Acta Psychiatr Scand. 1990 May;81(5):432-6.
- Salmaggi P, Bressa GM, Nicchia G, Coniglio M, La Greca P, Le Grazie C. Double-blind, placebo-controlled study of S-adenosyl-L-methionine in depressed postmenopausal women. Psychother Psychosom. 1993;59(1):34-40.
- Fava M, Giannelli A, Rapisarda V, Patralia A, Guaraldi GP. Rapidity of onset of the antidepressant effect of parenteral S-adenosyl-L-methionine. Psychiatry Res. 1995 Apr 28;56(3):295-7.
- Bell KM, Potkin SG, Carreon D, Plon L. S-adenosyl-L-methionine blood levels in major depression: changes with drug treatment. Acta Neurol Scand Suppl. 1994;154:15-8.
- Delle Chiaie R, Pancheri P, Scapicchio P. Efficacy and tolerability of oral and intramuscular S-adenosyl-L-methionine 1,4-butanedisulfonate (SAMe) in the treatment of major depression: comparison with imipramine in 2 multicenter studies. Am J Clin Nutr. 2002 Nov;76(5):1172S-6S.
- Pancheri P, Scapicchio P, Chiaie RD. A double-blind, randomized parallel-group, efficacy and safety study of intramuscular S-adenosyl-L-methionine 1,4-butanedisulphonate (SAMe) versus imipramine in patients with major depressive disorder. Int J Neuropsychopharmacol. 2002 Dec;5(4):287-94.
- Berlanga C, Ortega-Soto HA, Ontiveros M, Senties H. Efficacy of S-adenosyl-L-methionine in speeding the onset of action of imipramine. Psychiatry Res. 1992 Dec;44(3):257-62.
- Papakostas GI. Evidence for S-adenosyl-L-methionine (SAM-e) for the treatment of major depressive disorder. J Clin Psychiatry. 2009;70 Suppl 5:18-22.
*Article is from LifeExtension® (By David Hoffnung):
http://www.lifeextension.com/Magazine/2010/12/New-Human-Study-Confirms-Potent-Antidepressant-Effects-of-SAMe/Page-01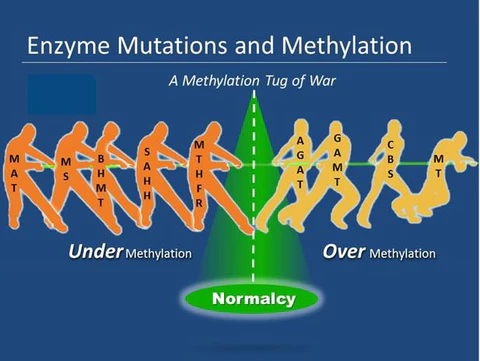
Difference undermethylated vs. overmethylated (symptoms)
According to Walsh Research Institute, nutritive support for treating underlying imbalances can be at least as effective for treating anxiety and depression as drugs (and without the side effects). As many as 85% with depression and 75% with anxiety in their massive database has reported significant improvement(1).
Many of the facts on this website https://VITAcure.me are based on the research of the non-profit organization Walsh Research Institute. For more information about the Walsh Approach, we encourage you to read the book “Nutrient Power” by the founder and President of the Walsh Research Institute, William J. Walsh, Ph.D., FACN.
Both for nutritive support and drugs, it is important to know about the underlying imbalance.Here is a comparison of undermethylated vs. over-methylated people to give you an idea of in which category you are. If you have some/more of the undermethylation symptoms and none/few of the over-methylation symptoms you are most likely in the undermethylation group of people. We might update this post with more symptoms/corrections. Many of the “problems” we can learn to live with and get used to of course, so with age some problems might diminish.
Undermethylated people tend to have more obsessive-compulsive tendencies (OCD) and controlling behaviour(2), addictiveness, and can also be quite aggressive. Severe, unshakable delusions, brain fog, etc. are also typical for under-methylators.
Even more information about undermethylation symptoms can be found in our blog post “How do you know if you are undermethylated?”.
Undermethylation Overmethylation Low pain threshold High pain threshold (shock resistant) Hot body temperature, profuse perspiration Low body temperature (hand/feet), sparse perspiration Mutations most likely to contribute to undermethylation are MTHFR (C677T especially, but also A1298C), MS, BHMT, MAT and SAHH Mutations most likely to contribute to overmethylation are AGAT, GAMT, CBS and MT Weak hair growth (men: beard/chest/arm), but little/no hairloss, difficulty building muscles, veins prominent Strong hair growth (men: beard/chest/arm – hirsutism), thick hair, but receding hairline with men, easily builds muscles High histamine, good response to antihistamines Low histamine, antihistamine intolerance No (few) food/chemical allergies, but seasonal inhalant allergies(2), air hunger, frequent colds, autoimmune diseases, urticaria/hives, frequent headaches, backaches, muscle cramps, chronic inflammations, peptic ulcers, irritable bowel syndrome, nosebleed, car sickness, history of miscarriage, women: mostly male offspring, cancer, early aging Several food/chemical allergies and absence of seasonal allergies(3), sleep disorder(3) Oily skin, acne, more salivary flow/tears (high fluidity)(2) Dry skin, eczema, dry mouth/eyes(3) Strong teeth Dental caries Low Homocysteine High Homocysteine Gloomy/catatonic Cheerful/grandiose Introvert/shy/oversensitive (especially as teenager), OCD (obsessions+compulsions), addictiveness, trichotillomania, ritualistic behaviour Extrovert, obsessions but not compulsions Calm demeanor(2), controlled, blank mind Outwards agitated/restless, stuttering, racing thoughts, hyperactivity(3) Not showing emotions, silent Can not hide emotions, think as they speech, pressure of speech, verbose, talkative Chronic/severe depression (but denial), suicidal tendencies, generalized anxiety* (too little serotonin: anxiety and depression can be a result of both under-, and over-methylation, so look at other symptoms to determine status) Periodic depression, self-mutilation, frenetic activity, restless legs/pacing(3), high anxiety(3); panic tendency(3) Lack of empathy (100% of psychopaths are undermethylated) Excellent socialization and very/over empathic(3) Antisocial-Personality Disorder, loner, resisting attention, social isolation, Conduct Disorder Social, enjoys attention from others, Episodic Rage Disorder Very competitive (especially in sports/games)(2), very strong-willed; oppositional to authority(2), high accomplishment when not ill, self-motivated Non-competitive in sports/academics(3) Inner tension(2), phobias, not satisfied with own body (can lead to Anorexia), perfectionist, low self-esteem (but denial) Content with own looks, grandiosity, thinks good of themselves, high self-esteem Very high libido(2) (abnormal behavior/interest) Lower/no libido(3) Oppositional Defiant Disorder (especially as child/youth, but might continue) Not as oppositional as child/youth, hyperactive Not hitting notes (not musical), perhaps less musical interest* Hitting notes very well (musical), very interested in music (broad) Intrusive thought interfering with daily life, rumination about past events, can be schizoaffective Religiosity, hallucinations, dysperceptions, perhaps voices/psychosis/evil spirits (100% of chronic schizophrenics are overmethylated) Slow calculation, poor short time memory/concentration endurance, excels in science/business/right brain activity (also improves musical awareness*), creative Quick calculation of simple mathematics, good short time memory Denial (of symptoms/disease/illness), noncompliance (with therapies, treatment, medicine), dietary inflexibility, belief that someone is after them (also friends), conspirational theories Paranoia, belief that everyone thinks ill of them, despair Low serotonin/dopamine activity, good response to SSRI’s(2)* (and methionine/SAMe), adverse reaction to too much folic acid, low tolerance for alcohol Elevated serotonin/dopamine activity, improvement after lithium, adverse reactions to antihistamines and SSRI’s(3)* (and methionine/SAMe) *Different responses to SSRIs: undermethylators have too little serotonin, and overmethylators have too much.
Walsh states that though SSRI’s may help (for undermethylators), side effects can be prohibitive, while nutritive support for underlying imbalances can be at least as effective(5).
If given to the wrong biotype SSRI’s can have fatal consequences (especially with young males). Please read this PDF: “A Proposal for Prevention of School Shootings” (by William J. Walsh).
The Incidence of Undermethylation (According to Walsh Research Institute’s research)(4):
- 98% of those on the Autism Spectrum clients at the Walsh Research Institute are undermethylated
- 95% of those with Antisocial Personality Disorder are undermethylated
- 90% of those with Schizoaffective Disorder are undermethylated
- 85% of those with Oppositional – Defiance are undermethylated
- 82% of those with Anorexia are undermethylated
- 38% of those with Depression are undermethylated
(Ref.: Walsh, William J. Nutrient Power. New York: Skyhorse Publishing, 2012)
References:
Symptoms are from:
Walsh Research Institute:
https://www.walshinstitute.org
and Books:
Nutrient Power: Heal Your Biochemistry and Heal Your Brain
By William J. Walsh, PhD, FACNNatural Healing for Bipolar Disorder: A Compendium of Nutritional Approaches
By Eva Edelman (Author), Abram Hoffer (Foreword)Numbered reference list:
1. https://www.walshinstitute.org/uploads/1/7/9/9/17997321/methylation_epigenetics_and_mental_health_by_william_walsh_phd.pdf [page 8]
2. https://www.walshinstitute.org/uploads/1/7/9/9/17997321/methylation_epigenetics_and_mental_health_by_william_walsh_phd.pdf [page 26]
3. https://www.walshinstitute.org/uploads/1/7/9/9/17997321/methylation_epigenetics_and_mental_health_by_william_walsh_phd.pdf [page 27]
4. https://www.walshinstitute.org/uploads/1/7/9/9/17997321/methylation_epigenetics_and_mental_health_by_william_walsh_phd.pdf [page 16]
5. Walsh, William J. Nutrient Power. New York: Skyhorse Publishing, 2012
(Please let us know if you are looking for a reference to a specific part, and we will add it to the list).
Methylfolate – the “suicidal” nutrient (don’t believe the hype)
Large doses of methylfolate should be avoided for undermethylated depressives (it will make depression worse), only a small dose is beneficial when you are undermethylated (we all need some folate, but too much can make you feel worse).
High doses of L-methylfolate (or folic acid) should only be given to overmethylated people with low folate. L-methylfolate is claimed to be a more bioavailable form than folic acid, so large doses of folic acid might not be absorbed in once. For instance, the Deplin brand of l-methylfolate is used in the following situations:
- In people with a major depressive disorder who have folate deficiency. Deplin is used together with antidepressant medications in people with major depressive disorder and low folate levels. (Comment: this is NOT for undermethylated people who usually always have high folate levels, but for overmethylated people who usually have low folate levels).
- In people with schizophrenia who have hyperhomocysteinemia related to folate deficiency. (Comment: it is always overmethylated people who have schizophrenia, not to be confused with schizoaffective, and it is usually only overmethylated people who have hyperhomocysteinemia (too much homocysteine)).
There are two reasons you should not take too much if you are undermethylated:
1. Folate tends to accumulate and trap methyl. As long as you supplement or get only the folate from your diet that you actually use, it is helpful, but if you supplement, or eat too much folate-rich food, it will build up and actually slow down methylation if there is not enough methyl available. Usually, under-methylators are high in folate, so to begin with folate should be avoided. Start with only SAM-e or with a very slow introduction of VITAcure Methyl Plus in addition to SAM-e. SAM-e is the jolt you need to kickstart the methylation cycle.
2. Even more important than the first reason is that folate act as a serotonin reuptake promoter. Serotonin reuptake is a far more dominant factor than the amount of serotonin present. And this is what you will read in this article.
3 Tablets of VITAcure Methyl Plus only contains 50mcg of methylfolate (in comparison ½ cup boiled spinach contains 131mcg folate). The amount methylfolate in Methyl Plus is that low for the purpose of not affecting serotonin re-uptake, and you better be careful with those folate-rich foods! If you are looking for recipes, here are some that are low in folate: https://www.samanthagilbert.com/recipes/recipes-undermethylation/
Also, check folate-rich foods and do not overdo the use of those on a daily basis. B-complex supplements often are high in folate and should be avoided (multivitamins/B-complexes often do more harm than good due to ingredients you should avoid taking too much of – so be careful).
Methylfolate is slightly better than folic acid and folinic acid for under-methylators, but one should be very careful if the goal is to avoid depression.
…”methylfolate act as serotonin reuptake promoter by an epigenetic mechanism, the opposite of what is needed.”
…”the reliability of genetic testing for assessing methylation is quite limited at present. Identifying SNP weaknesses in MTHFR and other methylation-cycle enzymes do not necessarily mean that the individual is undermethylated. There is a “tug-of-war” competition between enzyme SNPs that weaken methylation and SNPs in the SAMe utilization pathway that can produce over-methylation. Since the genetic information is qualitative and not quantitative, it is often impossible to determine the net methylation potential from genetic testing. Fortunately, there are blood tests that can test for overall methylation status.”…
…”Methylfolate is what I call a “suicidal” nutrient, that is, a nutrient that acts only once. After a single pass through a portion of the cycle, methylfolate loses its identity and becomes part of the garden-variety THF pool. Methylfolate is somewhat more effective than folic acid and folinic acid, but is not as effective as advertised.”
…”blindly using methylfolate for patients with 677T MTHFR or other weakened enzymes can produce negative results….tend to drive serotonin activity even lower by an epigenetic mechanism.”
Some still recommend methylfolate for depressive people with MTHFR. Read why that is wrong if serotonin activity is low (as with under-methylators – high folate biotypes) in this interview with William Walsh, where these quotes are from:
WILLIAM WALSH, Ph.D. (interviewed)
Many of the facts on this website https://VITAcure.me are based on the research of the non-profit organization Walsh Research Institute. For more information about the Walsh Approach, we encourage you to read the book “Nutrient Power” by the founder and President of the Walsh Research Institute, William J. Walsh, Ph.D., FACN.
You can read the original interview here (from Latitudes.org):
http://latitudes.org/dr-william-walsh-autism-ocd-pandas-depression-methylation/
Sheila Rogers DeMare: Dr. William Walsh, the founder, and president of the Walsh Research Institute is an international expert on nutrient-based psychiatry, including approaches to methylation. We posed several questions to him that had been received from our readers and he was kind enough to reply. He is a member of our ACN Latitudes advisory board, and we greatly appreciate his time and expertise. See WalshInstitute.org
Do you think autism is reversible, and if so, what approach does your research suggest would be most effective?
Dr. Walsh: Autism is very treatable and complete recovery is possible in young persons whose brains have not completed the early development process. I‘ve worked with thousands of patients with an autism spectrum disorder and seen hundreds who achieved full recovery after biochemical therapy and a special diet. Early intervention is essential. We can make more progress in a month with a two-year-old than in six months with an eight-year-old. It’s becoming increasingly clear that autism is an epigenetic gene-regulation disorder in which environmental insults alter DNA methylation.
Treatment success requires powerful antioxidant therapy, a toxin-free environment, and coping with G.I. tract problems. I believe the greatest progress can be made with brain-directed therapies that promote the development of brain neurons and synapses to enable improved cognition, speech, and socialization. My personal favorite is metallothionein-promotion therapy.
Many of our readers deal with obsessive-compulsive disorder (OCD). Would you please summarize the role of histamine in OCD.
Dr. Walsh: More than 90% of OCD patients are undermethylated with low neurotransmission at serotonin and dopamine receptors. In addition, many have low activity at N-methyl-D-aspartate (NMDA) receptors.
For years we have used whole blood histamine as a laboratory marker for methylation status. Another good lab test for methylation status is the SAMe/SAH ratio test offered by Doctors Data, Inc. Neither of these lab tests is perfect, but they are more reliable than present genetic testing for determining if a patient is undermethylated, over-methylated, or in the normal range.If someone seems to have symptoms of low histamine, are there ways to increase histamine levels? And if histamine is too high, what should be done.
Dr. Walsh: About 30 years ago, the great Carl Pfeiffer, MD, Ph.D., believed that histamine’s role as a brain neurotransmitter was a central factor in schizophrenia and other mental disorders. Since Pfeiffer’s death in 1988, we’ve learned this is not correct and that methylation imbalances (a) cause abnormal histamine levels and (b) have a major epigenetic effect on mental health. Methylation is the primary process for metabolizing (destroying) histamine and there is a convenient inverse relationship between histamine levels and methylation status. Our treatments are not aimed at normalizing histamine, but in dealing with the brain disorders associated with over-methylation or undermethylation.
Nutrient therapies for treating undermethylation are well known, but great care must be used in the case of undermethylated persons with low serotonin activity. Folic acid, folinic acid, and methylfolate all act as serotonin reuptake promoters by an epigenetic mechanism, the opposite of what these patients need.
There is increasing evidence that folates act as deacetylase inhibitors that enhance gene expression of SERT reuptake proteins known as “transporters”. Serotonin reuptake is a far more dominant factor than the amount of serotonin present. Folate supplements (together with B-12) are very effective in improving methylation in most undermethylated persons. However, folate supplements should be avoided for undermethylated patients who suffer from depression, anxiety, or other mental disorders that involve low activity at serotonin receptors.
Recent advances in epigenetic science have provided a roadmap for effective natural therapies that can regulate the activity of serotonin, dopamine and other neurotransmitters without the side effects associated with antidepressant drugs. I believe that the need for drug therapies will gradually fade away as brain science advances.
Have you seen any children with a PANDAS/PANS diagnosis, and do you think there is a nutritional way to avoid or treat such severe behavioral and neurological reactions to bacterial, viral, or other types of infections?
Dr. Walsh: PANDAS/PANS has many characteristics of an epigenetic gene-regulation disorder especially (a) sudden onset, (b) a multitude of serious symptoms, (c) a condition that is difficult to treat, and (d) a condition that can persist for years after onset. Epigenetic disorders are caused by environmental insults that alter DNA methylation or other gene-regulation factors.
I’ve only seen a few dozen children diagnosed with PANDAS and do not consider myself an expert in this disorder. I have noticed that most of these children exhibit severe undermethylation and oxidative stress. Also, a high percentage had elevated pyrroles and zinc deficiency. It’s hard to believe that nutrient therapies to correct these imbalances would not result in significant improvement. However, I have no outcome data for PANDAS/PANS.
Your research shows there are five types of depression, and you recommend that a different treatment approach should be taken for each type. How should a parent go about finding a doctor who can evaluate them to learn which type of depression they may have, and then offer suitable treatment?
Dr. Walsh: We have identified five chemical biotypes of clinical depression that represent about 95% of cases. Our classification system is based on studies of 2,800 patients, including more than 250,000 blood/urine chemistry results and in-depth medical history. Until now, most mainstream experts have regarded depression as a single condition with variations along a central theme – low activity at serotonin receptors.
We have observed low serotonin activity in two of the biotypes, with different brain disorders dominating the other cases. We reported these findings at the annual American Psychiatric Association (APA) meeting in New York City this spring.
The undermethylation (38%) and pyrrole disorder (15%) biotypes involve low serotonin activity with many reports of improvement after SSRI antidepressants. However, these patients also respond to individualized nutrient therapy. High-copper (17%) depressives showed little response to antidepressants but reported great improvement after copper-lowering nutritional supplements. The low-folate (20%) biotype consisted of patients who reported severe intolerance to SSRIs but thrived on supplements of folates and B-12. The smallest biotype (5%) involved toxic metal overloads such as lead, mercury, cadmium, etc.
At the APA we recommended inexpensive blood/urine tests for all depression patients, and different treatment approaches for each biotype. This is a medical procedure that requires a practitioner experienced in these protocols. We are actively engaged in continuing medical education (CME) educational programs to enable doctors to incorporate these methods into their practices.
Our next USA training program will be this October in Illinois. A list of doctors using these protocols is provided on our website and in the appendix of my book Nutrient Power.
In your opinion, do people fall into either an over-methylated or undermethylated status or can you be an under-methylator in certain areas of the methylation cycle and an over-methylator in other areas of the cycle? If someone has some traits of an under-methylator and some traits of an over-methylator, what would you recommend?
Dr. Walsh: Based on my massive chemistry database, about 22% of the population is undermethylated and 8% over-methylated. These are inborn tendencies that usually persist throughout life. Undermethylation usually results from single nucleotide polymorphisms (SNPs) that weaken MTHFR or other enzymes in the methylation cycle. Overmethylation is generally caused by enzyme weaknesses (SNPs) in the SAMe utilization pathways.
Nutritional supplements, certain drugs, and special diets can adjust methylation, but the inborn tendency usually remains. We have evaluated the methylation status of more than 25,000 patients and controls and identified dozens of distinctive symptoms and traits associated with methylation imbalances. For example, most under-methylators report allergies to ragweed and have a history of strong will, perfectionism, competitiveness, and OCD tendencies.
Overmethylators are usually characterized by excellence in music and art, empathy,
 excellent socialization, high anxiety, and food/chemical sensitivities. All of these traits are generalities with many exceptions and very few persons exhibit all of the traits associated with their methylation biotype. However, an experienced practitioner can usually predict the methylation lab results after a good medical history. Graphic: Courtesy of the Walsh Research Institute.
excellent socialization, high anxiety, and food/chemical sensitivities. All of these traits are generalities with many exceptions and very few persons exhibit all of the traits associated with their methylation biotype. However, an experienced practitioner can usually predict the methylation lab results after a good medical history. Graphic: Courtesy of the Walsh Research Institute.What are your thoughts on using genetic testing, such as “23 and Me” to create an individual methylation roadmap/treatment plan?
Dr. Walsh: Genetic testing is quite inexpensive, highly accurate, reliable, and will certainly grow in importance in future years. These tests can already identify predispositions for many disorders such as breast cancer and Alzheimer’s and may soon obsolete the need for pap smears. However, the reliability of genetic testing for assessing methylation is quite limited at present. Identifying SNP weaknesses in MTHFR and other methylation-cycle enzymes does not necessarily mean that individual is undermethylated. There is a “tug-of-war” competition between enzyme SNPs that weaken methylation and SNPs in the SAMe utilization pathway that can produce over-methylation.
Since the genetic information is qualitative and not quantitative, it is often impossible to determine the net methylation potential from genetic testing. Fortunately, there are blood tests that can test for overall methylation status (the net effect of the competing SNPs), and I greatly prefer to use them – SAMe/SAH ratio and whole-blood histamine. In addition, blindly using methylfolate (Deplin) for patients with 677T MTHFR or other weakened enzymes can produce negative results in patients afflicted by low serotonin activity. Folate supplements including Deplin tend to drive serotonin activity even lower by an epigenetic mechanism (see the third question, above).
The benefits from improving methylation are overwhelmed by weakened serotonin neurotransmission in these persons. Methylfolate supplements are a clever approach for coping with undermethylation in persons with MTHFR enzyme weaknesses. However, the potency of methylfolate has been greatly exaggerated. The methylation cycle spins constantly with more than a million methylation reactions per second.
The methylation cycle somewhat resembles the Indianapolis Speedway with traffic constantly spinning around the track. Methylfolate is what I call a “suicidal” nutrient, that is, a nutrient that acts only once. After a single pass through a portion of the cycle, methylfolate loses its identity and becomes part of the garden-variety THF pool. Methylfolate is somewhat more effective than folic acid and folinic acid but is not as effective as advertised. The bottom line is that methylfolate and other folate supplements are very effective in enhancing methylation for autism and other conditions that are not dominated by low serotonin activity.
In your book Nutrient Power, you frequently use the term “methyl” as in the methyl/folate balance and in giving methyl to address neurotransmitter imbalances. What is methyl? Do you mean methylcobalamin?
Dr. Walsh: The occasional use of methyl in my book is shorthand for methyl donors such as methionine and SAMe. Twenty years ago I presented a paper at the annual APA meeting describing the opposite effects of folate supplements and methyl donors on neurotransmitter activity and began using the term methyl/folate ratio. I believe it’s time to find a better expression for this factor.
Why not only SAM-e?
Most under-methylators are low in “everything” (homocysteine, SAMe, methionine, B6, Calcium, Magnesium, Zinc, Glutathione, Creatine, etc.) and what they need is more methyl. VITAcure Methyl Plus contains “everything” except SAM-e. An exception to this is folate: folate is essential in the methylation cycle*, but under-methylators are often too high in folate, and folate tends to accumulate and trap methyl, so avoid supplementation of high dose (but some is eventually necessary)!
Initially, homocysteine is TOO LOW with under-methylators. That could cause some problems since SAM-e converts from Methionine in our cells, which again converts from homocysteine. When there is not enough homocysteine, there will be problems creating enough methionine, etc. One should however not supplement directly with homocysteine, but start with SAM-e which again converts to homocysteine (therefore it is important to start with SAM-e before, or at the same time as carefully introducing VITAcure Methyl Plus).
There are of course other supplements that are helpful for under-methylators. For instance inositol (may reduce anxiety, promote sleep, critical to signaling, counterbalances choline, supports folates, B6, B12, TMG, and methionine). Tryptophan (serotonin support – helps balance mood and is often depleted). Both of these make you very sleepy, so you are better off taking these before sleep.
You could have problems converting homocysteine back to SAM-e quick enough. Supplementing with SAM-e will solve the initial problem of lacking SAM-e which is the principal methyl (CH3) donor in all cells of the body. The release of methyl increases, which you will notice giving you plenty of advantages if you are low (read: undermethylated).
SAM-e converts to SAH (S−Adenyl Homocysteine) by giving away a methyl group (CH3). And SAH is quickly transformed into homocysteine (HCY), which is more stable than SAH. Then HCY is converted back to SAM-e via B12/folate/TMG pathways. We all have this cycle in our cells. It takes place more than a billion times per second in the body. That should give you some idea of how important methylation is. If it did not happen, we would not be alive, but the SPEED of this process vary from one individual to another. Higher SPEED results in more methyl (CH3).You can end up with a higher level of homocysteine if you only supplement with SAMe unless you also provide the cofactors to help conversion back to SAMe. Check the risks (vascular problems etc.)! And you don’t want heart attacks, strokes, and even Alzheimer/dementia.
Be aware if you have high homocysteine levels before you try SAMe. Most undermethylated people have low homocysteine (contrary to what many people think) due to a slower methylation cycle, so that should not be a problem for most people. High levels of homocysteine results in narrowing of blood vessels, and small concentrations the opposite.
If the cells convert homocysteine back to methionine or cysteine more efficiently via different pathways, you can avoid the problem of homocysteine buildup, and more SAM-e is produced in your cells, reducing the need of supplementing with SAM-e after a while. And this is where VITAcure® Methyl Plus™ plays an important role, facilitating all the pathways, and also helping the cells to speed up the methylation cycle.
Some tend to think methylfolate alone will solve the problem. The problem is that folate is usually already high with histadelics (under-methylators), and it can cause symptom flareups, as (along with B12) it can increase the trapping of methyl molecules, so they need to restrict folate (B complexes are often too high in folate).
There are many other cofactors required. However, we will not go into detail explaining everything here. For instance, Magnesium is critical in metabolizing methionine to SAM, and absorbable form is crucial (avoiding aspartate or -glutamate). Calcium releases, and so lowers, histamine. Deficiency can directly cause histamine elevation. Calcium also supports catecholamine release into the synapse and is often depleted with under-methylators. Zinc counters overstimulation and supports homocysteine metabolism to cysteine or methionine, and is often depleted with under-methylators and even more so with pyrolurics. Zinc methionine is one of the two bio-available forms and the best choice for under-methylators and is for instance needed for synthesis of GABA in brain. Glutathione is needed to create homocysteine from SAH, and to methylate B12, so it can turn homocysteine to methionine, and is depleted by oxidative stress. Vitamin B-6 is an essential co-factor in synthesis of serotonin and in metallothionein formation, it also helps metabolize homocysteine to cysteine (we use the active form P5P coenzymated B6). Selenium (antioxidant support) from yeast is the best form of selenium. Vitamin C is an important antioxidant that decreases histamine, moderates stimulation and also antidepressant. Riboflavin 5-Phosphate is the bioactive, tissue ready form of riboflavin, which is an essential cofactor for the formation of other B vitamins, and necessary for methylation pathways in the body. NAD is used in the methylation cycle and is also directly involved in neurotransmitter production.
 Creatine is produced naturally in the human body. As much as 70%(1) of the SAMe is used in the creatine synthesis. Creatine is necessary for maintaining both muscle and brain tissue. Careful supplementation of creatine could help you even more with increasing methylation/SAMe, and at the same time give you other benefits both for muscles and your brain where the demand for creatine is high.
Creatine is produced naturally in the human body. As much as 70%(1) of the SAMe is used in the creatine synthesis. Creatine is necessary for maintaining both muscle and brain tissue. Careful supplementation of creatine could help you even more with increasing methylation/SAMe, and at the same time give you other benefits both for muscles and your brain where the demand for creatine is high. *Methylation cycle (Methionine->SAMe->SAH->Homocysteine->Methionine…):
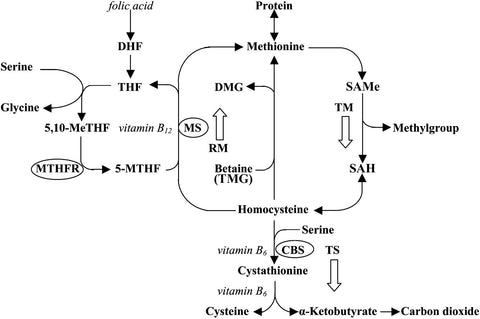
A concise overview of homocysteine metabolism, with open arrows indicating metabolic fluxes, ovals indicating enzymes and italics indicating vitamins. Homocysteine is the transmethylation (TM) product of the essential sulphur-containing amino acid methionine, with SAMe and SAH as intermediates. Homocysteine can be either remethylated to methionine or degraded by trans-sulphuration (TS). In the folic-acid-dependent remethylation reaction, which is catalyzed by methionine synthase (MS) and uses vitamin B12 as a cofactor, 5-methyltetrahydrofolate (5-MTHF) donates a methyl group to homocysteine. Subsequently, tetrahydrofolate (THF) receives a methylene group from the serine/glycine couple, a reaction that uses vitamin B6 as a cofactor. Tetrahydrofolate can also be generated by reduction of supplemented synthetic folic acid to dihydrofolate (DHF) and subsequently to THF. Next, 5,10-methylenetetrahydrofolate (5,10-MeTHF) is reduced to 5-MTHF, requiring the enzyme methylenetetrahydrofolate reductase (MTHFR). Another folic-acid-independent remethylation reaction, uses betaine (TMG) as a methyl group donor, generating dimethylglycine (DMG). In the irreversible catabolic (trans-sulphuration) pathway, the rate-limiting reaction is catalyzed by cystathionine β-synthase (CBS) and requires the active form of vitamin B6 as a cofactor.
Numbered reference list:
1. https://www.walshinstitute.org/uploads/1/7/9/9/17997321/methylation_epigenetics_and_mental_health_by_william_walsh_phd.pdf [page 21]How do you know if you are undermethylated?
Just because you have an MTHFR C677T/A1298C mutation doesn’t mean you’re over or under methylated (although it would be one factor that might push the balance to undermethylation). Dr. Walsh (Walsh Research Institute) describes one’s methylation status as being like a tug of war between opposing factors. Many of those are genetic, and some are nutritional or environmental.
According to Dr. Walsh’s research(1), 70% of the population are normal methylators, 22% are under-methylators, and 8% are over-methylators, but this again may depend on what you define as under/over-methylation/normal. Pfeiffer statistic says 45% are under-methylators and 15% are over-methylators (only 40% normal). This is just a matter of definition of the “normal” area. Undermethylation indicates that the methylation cycle as a whole slows down enough that the end product, SAMe, is typically inadequate and thus causes symptoms.
One and each of these symptoms is not a reliable indicator by it self since it could be caused by other factors. However, if you recognize most or many of these symptoms, being undermethylated might be the underlying problem. You might not have most of the symptoms of course, even if you are severely undermethylated. Look at symptoms first, then one can try supplementing with SAMe* for a while, and if that makes you feel better (and not worse) you should add the cofactors if you have not done so already. Blood test measuring SAM/SAH ratio is the most reliable lab-test. Genetic testing could give some hints, but does not provide any definite answers so far. 677T & 1298C mutations (methylenetetrahydrofolate reductase) could be a small clue, but one could be undermethylated without any mutation in these genes and vice versa. The presence of one or more of these mutations isn’t enough to say if you’re an over or under methylator. The combination of all of your genetic factors as well as your nutritional state must be taken into account. The best way to determine is through symptoms and traits, but again, you can be undermethylated even if you do not have most of the symptoms. Please also read this updated post about the difference between undermethylation and overmethylation.
*Be aware if you have high homocysteine levels before you try SAMe. Most undermethylated people have low homocysteine (contrary to what many people think), so that should not be a problem, to begin with for most people. High levels of homocysteine results in narrowing of blood vessels, and small concentrations the opposite.
Methyl (CH3) is the simplest organic molecule and is responsible for a vast number of functions in our body. Methyl is for instance used in DNA-methylation (protein production necessary for gene expression) and is also the essential component for formation of neurotransmitters controlling brain function. Therefore there will be some significant symptoms, both physical and psychological):
1. (Psychological) Depression, maybe mild. You might not be aware of it yourself since it has been like that all your life, even though other people enjoy life, social activities, music and laugh more than you. Getting up in the morning might not be one of your favorite things to do. Little energy. The reason is low levels of neurotransmitters.
2. (Both physical due to capillaries, and also because of being low on neurotransmitters): Low pain threshold (easily burned, etc.)
3. (Other psychological symptoms) Poor short-time memory* and not remembering dreams (due to lacking vitamin B6 and key neurotransmitters). High accomplishment and self-motivated (read: loner), very strong willed but poor concentration endurance, bouts of adrenal exhaustion. Shy, antisocial personality, infrequent and terse speech, obsessive-compulsive tendencies (OCD), intrusive/excessive thoughts interfering with daily life, oversensitive, phobias, inner tension, strong will, competitiveness (especially in sports and games), perfectionist, not satisfied with body, might wake up at night (easily woken), unwillingness/noncompliance to be treated/therapies (do it yourself), denial of illness (hiding problems), lack of empathy (psychopathic tendencies in severe cases), not showing emotions, catatonic, calm but inner tension, episodes of blank mind, oppositional as child/youth, cries easily, phobias, ritualistic behaviour, internal anxiety, rumination about past events, delusions, dietary inflexibility, high libido, easy orgasm, not hitting notes, not so interested in music. Same reason as above (low on neurotransmitters). High histamine and low serotonin, dopamine, and norepinephrine.
4. (Physical) High body temperature, profuse perspiration, heavy salivary flow/tears etc., strong teeth, prominent incisors, veins often prominent, more capillaries give you, for instance, quicker sunburn (depends on skin complexion), and frostbites. Sparse facial/body hair (beard/chest/arm/leg) with men (weaker hair growth). Acne*, early aging* (wrinkles, etc.), gray hair* and white spots* on fingernails (due to lacking Zinc/SAM-e). Maybe larger ears (growing due to excessive heat), long fingers and toes (depending on other genetics also). Prone to sneezing in sunlight, seasonal allergies (if high histamine), autoimmune diseases, cancer, respiratory allergies/asthma, rhinitis, hives, glue ear, osteoporosis, arthritis, cataracts, MS, lupus, headaches, backaches, muscle cramps (due to lacking magnesium), peptic ulcers, autoimmune disorders, anorexia and bulimia. Women give birth to mostly male offspring. Fast metabolism: might have a lean build despite hearty appetite (depending on other factors of course).
This list is not complete.
Due to mostly male offspring from women, most likely either your father only (mostly) had brothers or you mothers father only (mostly) had brothers. Then again the parent/grandparent who only had brothers had a mother that was undermethylated and then again had a father with only (mostly) brothers and so on (this is not 100% certain of course, but very likely). The undermethylated mother usually gives birth to male children because thin copious vaginal secretions foster the creation of males.
There are both benefits and disadvantages from being undermethylated, but correcting imbalances (especially undermethylation) will probably only be experienced as beneficial in many ways (chances of being over-methylated are small, and moving towards the “normal” area is only beneficial both mentally and physically).
Undermethylation is often combined with *Pyroluria caused by stress that depletes the body even more of vitamin B6, magnesium, and zinc (which is already quite low with under-methylators). If so, these symptoms can occur also: dry/pale skin, stretch marks, acne, acetonic breath/body odor, delayed growth puberty, inability to tan, sunburned, white spots on fingernails, early gray hair, frequent infections, morning nausea, hypersensitive to light and noise, poor sense of smell/taste, preference for spicy food, sensitive to gluten/casein, oxidative stress, stitch in side when running, extreme mood swings, poor stress control, overwhelmed of criticism, adverse to changes in routine, histrionic behaviour, impulsive, fatigue, less dream recall, problem with sugar metabolism, intolerance/sensitivity to some proteins/alcohol and others.
The over-methylator might have the opposite symptoms than many of these (high pain threshold, cold, heavy body hair, eczema, dry eyes and mouth, higher musical interest and extrovert, etc.). If that is the case, VITACURE® METHYL PLUS™ and SAMe is not for you. Undermethylation is much more widespread than over-methylation (about three times more common). Both biotypes struggle with addiction. The difference is the cause: over-methylators turn to drugs to try and suppress high anxiety or panic as a result of too much neurotransmitter activity, while under-methylators become obsessive compulsive with a substance or concept because of little neurotransmitter activity. The preferred drug might be different due to how they affect neurotransmitter activity.
Numbered reference list:
1. https://www.walshinstitute.org/uploads/1/7/9/9/17997321/methylation_epigenetics_and_mental_health_by_william_walsh_phd.pdf [page 14]
The new product: VITAcure® Methyl Plus™ is now in stock
February 2017: Finally our new and unique product: VITAcure Methyl Plus™ is in stock here in the US (Massachusetts) ready to be shipped today both within the US and to the rest of the world.
VITAcure METHYL PLUS is a specially tailored product for people who are undermethylated. To increase methylation, one might also want to take SAM-e. It is essential to take cofactors in addition to the methyl-donator SAM-e to get the methionine-cycle functioning as it should. Before this supplement was available, one would have to source a number of different nutrients in addition to SAM-e, but finally, there is one product that covers almost everything. For the under-methylator to get the methionine cycle to function properly, one will often have to take higher doses of nutrients not available in a regular healthy diet, and it is necessary to get those nutrients every day.
We manufacture the product in the US with the best available forms of nutrients and the highest possible quality in both the choice of nutrients and manufacturing process. VITAcure has developed this product in cooperation with the manufacturer: FoodScience of Vermont.